Case of an 82 years old female with knee joint pain
This is
an online e log book to discuss our patient's de-identified health data shared
after taking his/her/guardians' signed informed consent. This Elog reflects my
patient-centered online learning portfolio.
This is the case of an 82 years old housewife, resident of Bidar, Karnataka.
CHIEF COMPLAINT
The patient presented with
fever since 2 days
knee joint pain since 2 days
swelling in both legs below knee joint since 2 days
HISTORY OF PRESENTING ILLNESS
The patient was apparently asymptomatic 3 weeks ago, when in the morning after waking up ,the patient was unable to lift both her legs from the bed due to weakness and felt the heaviness of the legs. She recalls dragging herself to the bathroom.
3 days later, the patient developed swelling and pain in both lower limbs at and below the knee joint, right more than left. The pain was sudden in onset, pricking in nature, continuous, aggravated with walking, relieved on taking rest, and did not radiate to any other site. It was associated with redness and increased warmth of the overlying skin. The patient also complained of high-grade fever, that was continuous and not associated with chills and rigor, associated with generalized body pain.
The patient visited a doctor and was prescribed medication, after which her symptoms were reduced.
1 week ago the patient presented to our Hospital as her fever, swelling, and pain aggravated, medication was given and symptoms were reduced.
2 days ago, the patient presented back to the hospital with fever, bilateral knee joint pain, and swelling, more in the right leg than the left.
The patient also complains of pain in the joints of both hands since 15 days.
The patient also complains of bilateral knee joint pain while climbing stairs , that is relieved on rest .
HISTORY OF PAST ILLNESS
Known case of HTN since 13 years.
Not a known case
of DM, asthma, TB, Thyroid condition, CVD, or Epilepsy.
History of trauma 10 years ago, resulting in fracture of the left ulnar bone
History of syncopal attack 8 months ago.
No history of blood transfusion
DRUG HISTORY
Telmisartan and amlodipine since 13 years .
Ecosprin since 8 months
Diethylcarbamazine since 15 days.
Amoxycillin since 7 days .
FAMILY HISTORY
Brother and sister are known cases of asthma.
PERSONAL HISTORY
DIET- Vegetarian
APPETITE- Normal
SLEEP- Disturbed. Consuming alprazolam since 4 months
BOWEL
AND BLADDER MOVEMENTS -
Micturition - 4-5 months ago complained of low urinary output. Currently increased frequency of urination at night and reduced control in the bladder.
Bowel movements- Regular
ADDICTIONS- none
ALLERGIES-none
EXAMINATION
VITALS
PR- 94 bpm
BP- 120/70mmHg
AFEBRILE
GENERAL EXAMINATION
The
patient is conscious, coherent and cooperative.
She is moderately built and nourished
Pallor-
Present
Icterus-
Absent
Cyanosis-
Absent
Clubbing-
Absent
Lymphadenopathy-
Absent
Koilonychia-
Absent
Pedal
oedema- present
Peripheral pulse felt.







MUSCULOSKELETAL SYSTEM
Inspection
Bilateral swelling of the lower limbs, at and below the level of the knee joint. More prominent on the right than the left.
Right, Limb Fixed flexion deformity seen at the knee joint.
Left lower limb, ability to flex knee present.
No scars, sinus, erythema or rashes
Palpation
Local rise of temperature present bilaterally on the knee joint
Palpable swelling is present on the right and left knee, and ankle with mild oedema in her lower limbs , associated with tenderness, in the suprapatellar bursa
Patellar tap is positive bilaterally.
Join Line tenderness observed.
absence of lower limb shortening.
Range of motion
Inability to flex the left lower limb.




Provisional Diagnosis
? Bursitis
? Osteoarthritis
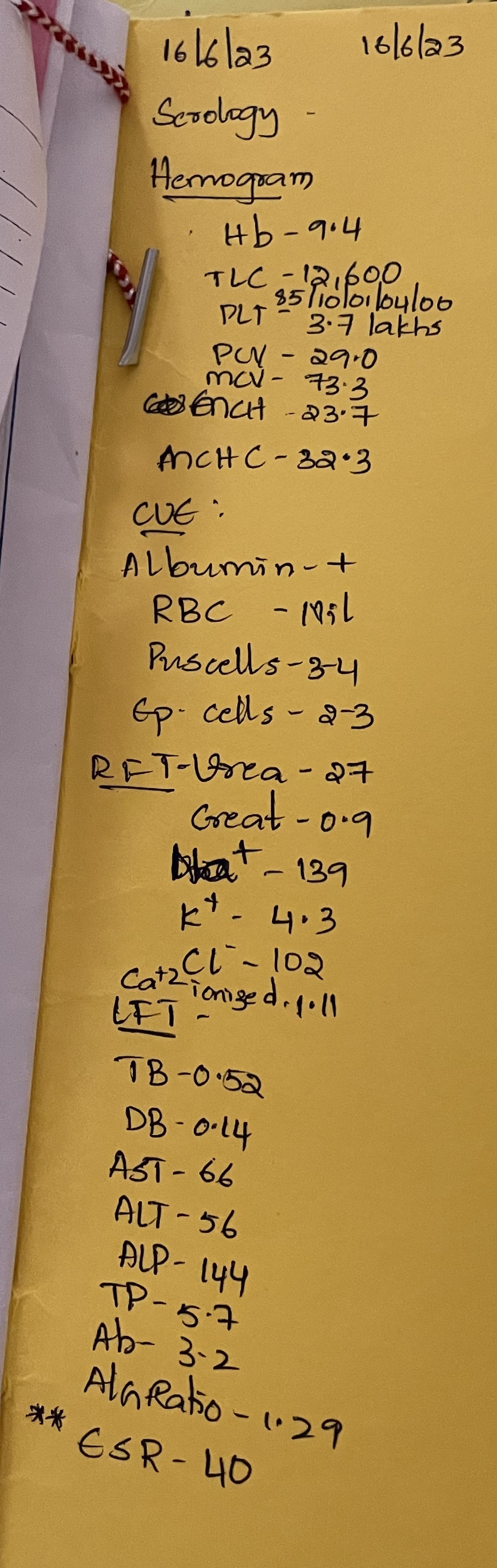
INVESTIGATIONS










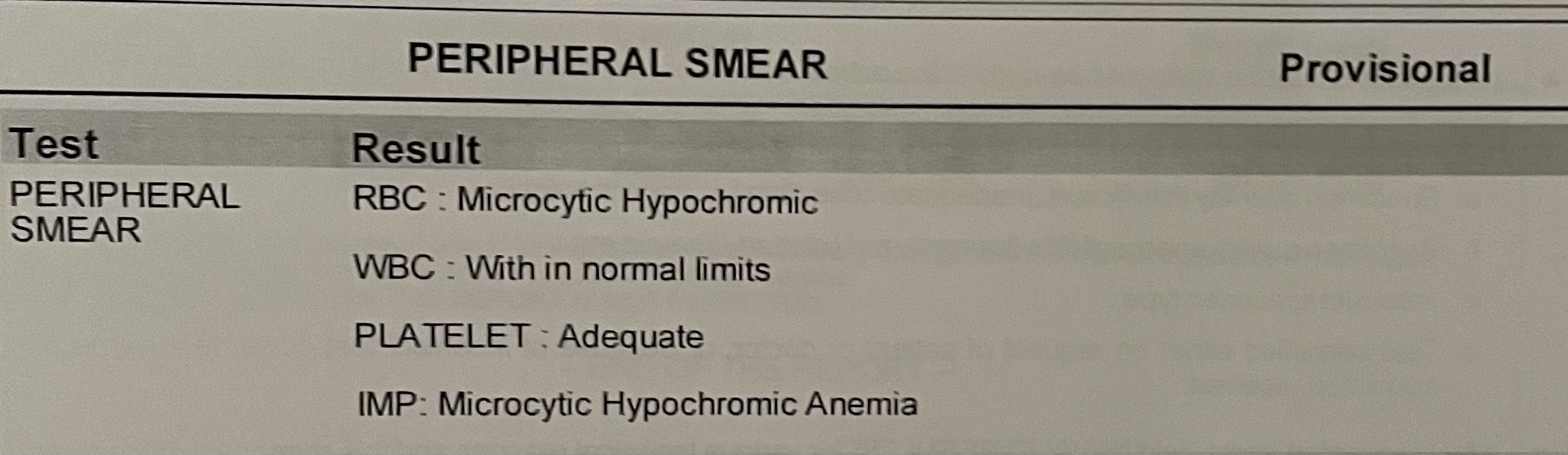






16/6/23











 .
.




20 days after second discharge
the patient presented to the causality again with chief complaints of
Fever and generalised body weakness , both since one day.
History of Present Illness
The patient was apparently asymptomatic 1 day ago , when she developed fever in the evening. Which was sudden in onset ,continuous , high grade (104 degree F). It increased at night after which the patient was brought to the casualty. It was relived on taking paracetamol (Dolo 650). No aggravating factors , not associated with chills and rigour.
Since the onset of fever, the patient also experienced generalised body weakness.Which was gradual in onset and progressive in nature. The patient was unable to get up from the bed and a described a feeling of heaviness in the legs.




Diagnosis :
Pyrexia with polyarthralgia with iron deficiency anemia

Comments
Post a Comment